
Buttock and Hip Pain:
When It’s Really from the Sacroiliac (SI) Joint

Many people who experience pain in the buttock or hip assume the problem lies in the hip joint itself. In reality, the source is often the sacroiliac (SI) joint where the spine connects to the pelvis. This joint plays a key role in supporting movement and weight transfer, and when it becomes irritated, it can cause deep, radiating pain that mimics other conditions.
What Is the SI Joint?

The SI joint connects the base of your spine (sacrum) to the two large pelvic bones (ilia). It’s designed for limited motion
and stability. Inflammation, wear, or injury can cause pain in the lower back, buttock, or even down the leg.
How SI Joint Pain Feels

Deep aching pain on one side of the lower back or buttock
Pain that radiates to the hip or groin
Worsens when standing, climbing stairs, or getting out of a car
Improves when lying down
Sometimes confused with lumbar disc or hip joint pain
Because symptoms overlap, precise diagnosis is crucial.
Common Causes

Injury or trauma (e.g., fall or accident)
Pregnancy or childbirth (ligament laxity and pelvic stress)
Leg length differences or gait changes
Arthritis or joint degeneration
Prior spine surgery altering load on the SI joint

Common Causes
Injury or trauma (e.g., fall or accident)
Pregnancy or childbirth (ligament laxity and pelvic stress)
Leg length differences or gait changes
Arthritis or joint degeneration
Prior spine surgery altering load on the SI joint

Diagnosing SI Joint Pain
A detailed exam helps distinguish SI pain from lumbar or hip problems. Evaluation may include:
Physical maneuvers reproducing pain (e.g., FABER test)
Imaging (X-ray, MRI) to rule out other causes
Image-guided SI joint injection the most accurate diagnostic tool
If pain relief follows an SI injection, the diagnosis is confirmed.
Diagnosing SI Joint Pain
A detailed exam helps distinguish SI pain from lumbar or hip problems. Evaluation may include:
Physical maneuvers reproducing pain (e.g., FABER test)
Imaging (X-ray, MRI) to rule out other causes
Image-guided SI joint injection the most accurate diagnostic tool
If pain relief follows an SI injection,
the diagnosis is confirmed.
Effective Non-Surgical Treatments

Image-Guided SI Joint Injection
A precise injection of anti-inflammatory or orthobiologic material reduces irritation and improves mobility.
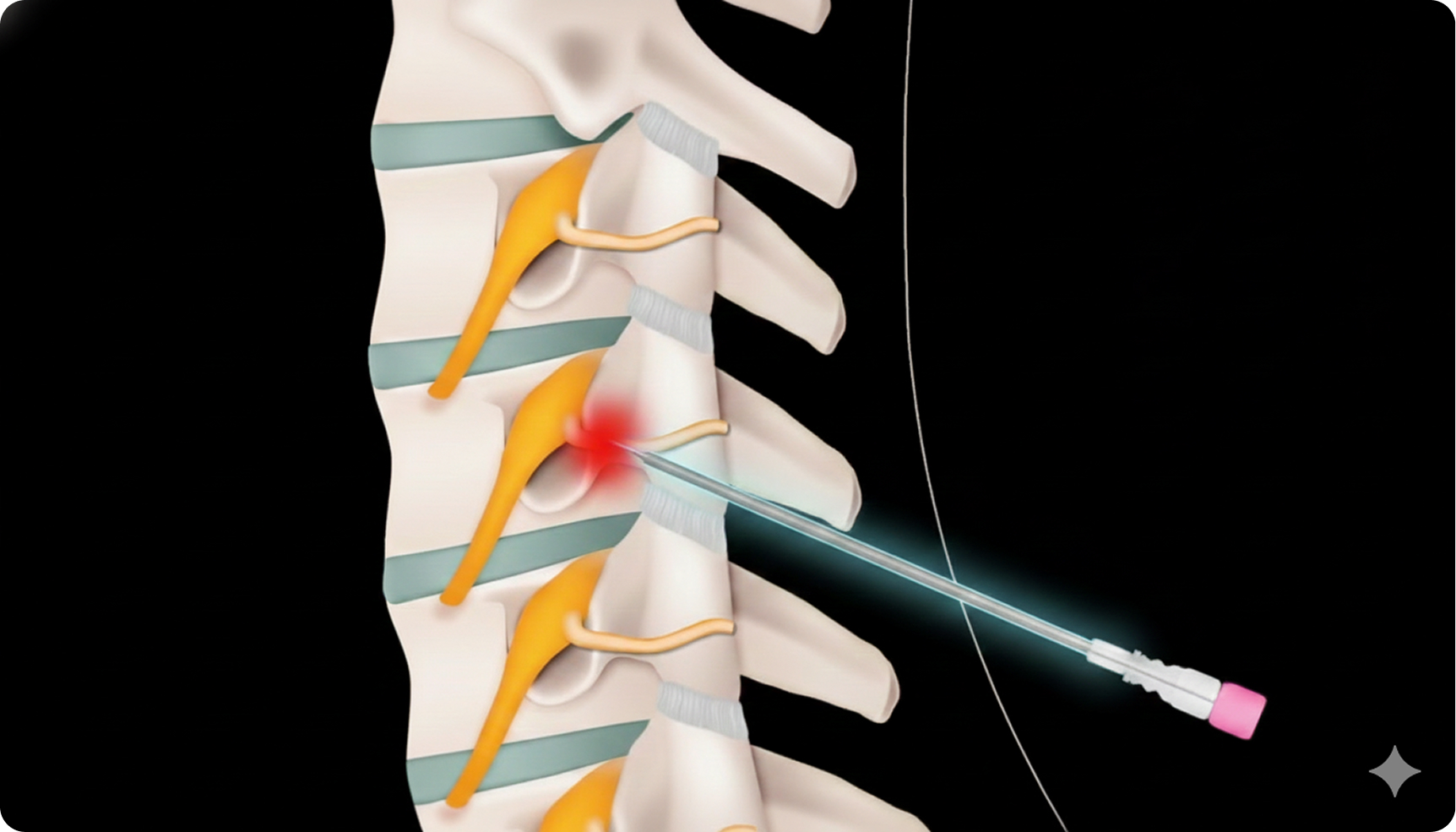
Radiofrequency Ablation (RFA)
Disrupts pain signals from the small nerves serving the jointoften providing relief lasting 6–12 months.

PRP or Bone Marrow “Cell” Therapy
Uses your body’s own growth factors to promote joint healing and stability.
Frequently Asked Questions

01. What is a facet ablation (RFA), and how is it different from diagnostic blocks?
Answer: Blocks test the pain source; ablation stops the nerve signal.
A medial branch block temporarily numbs a spinal joint to confirm the pain generator. If it works, radiofrequency ablation (RFA) uses heat to deactivate that small nerve for 6–12 months. The joint stays stable, and pain often lessens dramatically.
02. How long does a radiofrequency ablation (RFA) last, and can it be repeated?
Answer: Relief often lasts 6–12 months and the procedure can be repeated safely.
After an RFA, the tiny sensory nerves that send pain signals grow back slowly. Many patients enjoy meaningful relief for 6 months to a year. If the pain returns, a repeat ablation can usually be performed using the same approach. Regular stretching and strengthening help extend the benefit.
03. Why does my low back hurt after sitting or long drives?
Answer: It’s usually from facet-joint stress or weak postural muscles.
Sitting flexes the lumbar spine and compresses facet joints and discs, especially if the core is de-conditioned. Over time, this posture leads to inflammation and stiffness. Supportive cushions, regular breaks, and targeted therapy for core and glute muscles often relieve symptoms.
04. What is a diagnostic discogram, and why is it rarely done now?
Answer: It injects dye into spinal discs to find the pain source but carries risks.
Discography involves pressurizing discs with contrast dye while monitoring pain response. It was once common before spine surgery but is now less used because it can worsen disc damage and cause infection. Modern MRI and targeted nerve blocks provide safer diagnostic insight.
05. Why do some people have chronic back pain even after “successful” fusion surgery?
Answer: Adjacent levels often wear out faster.
Spinal fusion stabilizes one level but transfers stress to the discs and joints above and below, leading to adjacent segment disease. Scar tissue, muscle atrophy, and nerve irritation can also persist. Nonsurgical options like PRP or radiofrequency treatment can help preserve the surrounding spine.
06. What are “adjacent segment disease” and “hardware failure” after spine surgery?
Answer: They mean nearby levels or implants break down over time.
After fusion, joints next to the fused area compensate by moving more, sometimes developing arthritis or stress fractures. Hardware fatigue or loosening can also occur years later. Regular imaging helps detect changes early; pain-management injections or strengthening programs can often delay revision surgery.
07. How do you tell if leg pain is from the back or from a knee or hip problem?
Answer: Back-related pain travels below the knee; joint pain usually stays local.
Nerve compression in the spine typically causes sharp, shooting pain that radiates past the knee or into the foot. Hip or knee arthritis usually creates aching localized pain or stiffness without tingling. Imaging and physical-exam maneuvers help determine whether the source is spinal, joint, or both.
08. What is an epidural steroid injection and what does it do?
Answer: It delivers anti-inflammatory medicine around pinched nerves.
Guided by X-ray, a thin needle places medication into the epidural space of the spine. The steroid reduces swelling around irritated nerves from a herniated disc or arthritis. Relief may last weeks to months and can allow better participation in physical therapy.
09. What are red-flag symptoms that spine pain is not just mechanical?
Answer: Fever, unexplained weight loss, numbness, or bladder issues.
Warning signs include constant pain at rest, night sweats, progressive weakness, loss of control of urine or stool, or recent infection. These could signal infection, tumor, or severe nerve compression and need emergency evaluation.
10. How long should I wait before considering spine surgery?
Answer: Only after conservative care has clearly failed and red flags are excluded.
Most mechanical back or neck pain improves with guided injections, therapy, or biologic repair within 3–6 months. Surgery is reserved for progressive weakness, structural instability, or nerve compression causing loss of function. A second opinion is always appropriate before proceeding.
11. What is a “facet joint,” and why can it cause back or neck pain?
Answer: It’s a small stabilizing joint behind each vertebra that can become arthritic.
Facet joints allow bending and twisting. With aging or injury, they may develop arthritis and inflammation that causes sharp localized pain, often worse when leaning backward or standing long periods. Facet injections or RFA can calm these joints for months at a time.
12. When should I seek emergency care after a neck or back injury?
Answer: Sudden weakness, numbness, fever, or bladder/bowel changes.
Go to the ER immediately for severe pain with loss of strength, incontinence, high fever, or trauma with head injury. These could indicate nerve or spinal-cord compression, infection, or fracture. Early treatment prevents permanent damage.
13. What is a “nerve root block,” and how is it different from an epidural?
Answer: A nerve-root block targets one specific nerve, while an epidural bathes several.
A selective nerve-root block (SNRB) uses live X-ray to deliver medication directly around one irritated spinal nerve. It helps confirm which nerve causes the pain and can calm inflammation at that precise level. Epidural injections are broader, covering multiple nerves at once.
14. How can I tell if my hip pain is coming from the joint or my back?
Answer: Hip arthritis hurts in the groin; back problems radiate to the leg.
Hip joint disease often causes deep aching in the groin or front thigh, worse with walking or stairs. Lumbar nerve compression tends to cause burning or tingling down the leg. Diagnostic injections into the hip or spine can confirm the true source.
15. Can regenerative medicine help spine patients who already have hardware or fusions?
Answer: Yes, but injections are placed around not into the fused levels.
PRP and bone-marrow concentrate can reduce inflammation in joints and ligaments next to a fusion where new pain develops. These procedures don’t interact with the hardware itself. Most patients benefit from improved flexibility and less reliance on pain medication.
Take the Next Step
Don’t let hip or buttock pain limit your movement. Modern, image-guided options can identify and treat the source precisely.
Minimally invasive spine & joint care.
This page is informational only. No medical advice. Book on our secure intake portal.
© 2026 Elite Pain and Health. All Rights Reserved.